
Summary
- People with low arches are 20 times more likely to be injured than people with neutral arches, while people with high arches are nearly 80 times more likely to be injured (1).
- Although effective at controlling motion and reducing injury rates, recent research shows custom orthotics can produce appreciable reductions in arch muscle volume (3,4).
- Our new Peel and Stick Varus and Valgus Posts are inexpensive and easy to use, and provide all of the benefits of orthotics without the risk of damaging the intrinsic muscles of the arch.
For more than 60 years, both custom and over-the-counter orthotics have been used for treating and preventing injuries in individuals with either high or low arches. Protecting this population from injury is important, as a 2019 study of 600 novice runners showed that runners with low arches were nearly 20 times more likely to be injured than runners with neutral arches, and runners with high arches were nearly 80 times more likely to be injured than neutral arched runners (1). Historically, these injuries have been successfully managed with both custom and over-the-counter orthotics, which have been proven to decrease the velocity and range of pronation, lessen tibial internal rotation, improve shock absorption, and decrease strain in the foot and ankle musculature (2). The high patient satisfaction rates and improved clinical outcomes associated with orthotic intervention explains why more than 80% of sports doctors routinely prescribe orthotics for their patient population.
There are, however, a few serious drawbacks to the widespread use of orthotics. One obvious downside is the cost: because of high laboratory fees and the time spent casting and dispensing orthotics, it’s not uncommon for doctors to charge $400 for a pair of custom orthotics. Another more significant problem is that orthotics can cause appreciable atrophy of the arch muscles. In 2016, McClinton et al. (3) evaluated toe strength in individuals with and without heel pain and determined that subjects with heel pain had weaker toes than the control group. Importantly, the authors noted that individuals who self-reported long-term orthotic use had the weakest toes. More recently, researchers from Canada used ultrasonography to measure arch muscle volume before and after a 12-week study in which young adults wore either custom orthotics or their normal footwear (4). At the end of the study, volume of the abductor hallicus muscles decreased by more than 17%, while the flexor digitorum brevis muscles decreased in volume by 10%. Atrophy of these muscles is extremely important as abductor hallicus atrophy correlates with the development of bunions, and flexor digitorum brevis atrophy correlates with the development of plantar fasciitis and impaired athletic performance (Fig. 1). Apparently, the excessive arch elevation present in cus- tom orthotics offloads the intrinsic arch muscles so effectively that these important muscles atrophy from disuse.
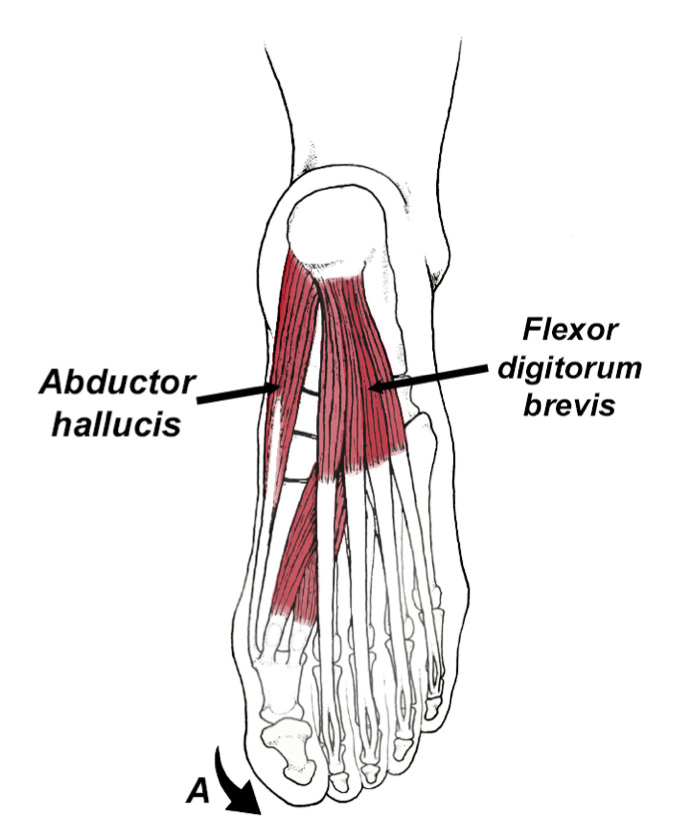
Fig. 1. Orthotic use has been shown to cause significant atrophy of abductor hallucis and flexor digitorum brevis muscles. Abductor hallucis weakness has been shown to correlate with the development of bunions (A), while atrophy of flexor digitorum brevis is associated with chronic plantar fasciitis and impaired athletic performance.
The obvious solution to prevent orthotic-induced weakness of the arch is to recommend strengthening exercises when prescribing orthotics. The problem with strengthening exercises is that they are time-consuming and compliance is low.
An inexpensive alternative to orthotics that does not risk weakening the arch is to prescribe varus and valgus posts that do not support the arch in any way. In the last few years, a growing body of research is showing that the simple addition of wedged insoles produces all the favorable advantages associated with orthotic intervention, without the risks associated with supporting the arch. For example, early research out of Japan showed that valgus wedges placed beneath the outer side of a patient’s insole reduced the adduction moment at the knee, significantly lessening discomfort associated with medial knee arthritis (5) (Fig. 2). More recent research has shown that valgus wedges reduce compression of the medial knee by 4 to 12% compared to barefoot or shoes alone (6,7,8). Patients who had the best responses to valgus wedges were younger, had a lower body mass index and presented with less severe arthritis (9,10). Post angles as low as 4° were shown to substantially reduce compression of the medial knee, and this low angle is unlikely to cause discomfort elsewhere in the kinetic chain (11).
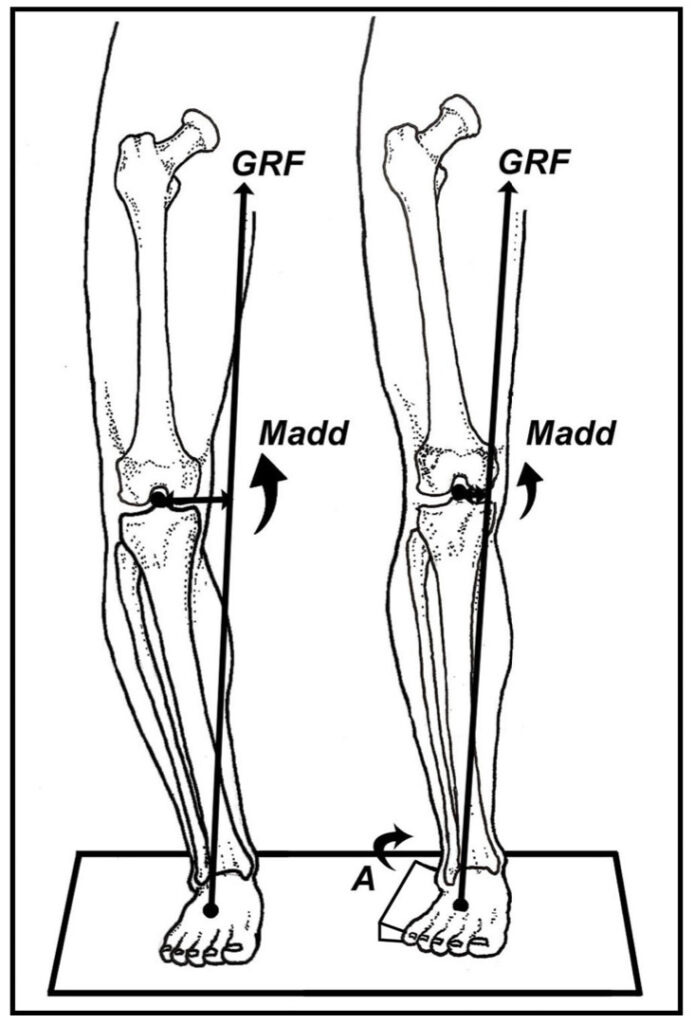
Fig. 2. A valgus post placed beneath the lateral foot (A) lessens the adductor moment arm generated at the knee (Madd). In addition to lessening symptoms associated with medial knee arthritis, valgus posts are often very effective in preventing ankle sprains in people with high arches. According to Hinman et al. (17), full length valgus posts are more effective than posts placed beneath the heels alone. Because medial knee arthritis has been shown to correlate with weakness of the hip abductors (18), in addition to valgus posts, all patients with medial knee arthritis should be evaluated for hip abductor weakness and aggressive hip strengthening should be pre- scribed when needed.
Valgus posting placed beneath the forefoot alone has also been shown to be an effective method of managing plantar fasciitis. To prove this, Kogler et al. (12) surgically inserted strain gauges into the plantar fascia of 9 cadaveric feet and placed angled wedges beneath the foot in a variety of locations before axially loading each foot with up to 900 newtons applied through the tibia. Strain gauge measurements revealed that placing an angled wedge beneath the lateral forefoot appreciably reduced strain in the plantar fascia by locking the calcaneocuboid joint thereby offloading the plantar fascia. Because valgus posts increase the range of rearfoot pronation, they are typically only used to manage plantar fasciitis in people with high arches.
Varus posting has also been proven to significantly improve lower extremity motion. Stackhouse et al. (13) demonstrate that varus posts placed beneath insoles reduce the overall range of rearfoot pronation, lessen internal tibial rotation, and decrease the velocity of knee flexion during stance. All of these biomechanical findings have the potential to greatly reduce the risk of knee injury. In another interesting study, Joseph et al. (14) had 10 female Division I college athletes perform a drop jump test while wearing a conventional flat insole, or an insole modified with a full-length 5° varus wedge. Subsequent three-dimensional motion analysis confirmed that the varus posts reduced knee valgus at initial contact, reduced the maximum knee valgus angle, and decreased ankle pronation during initial ground contact (Fig.3).
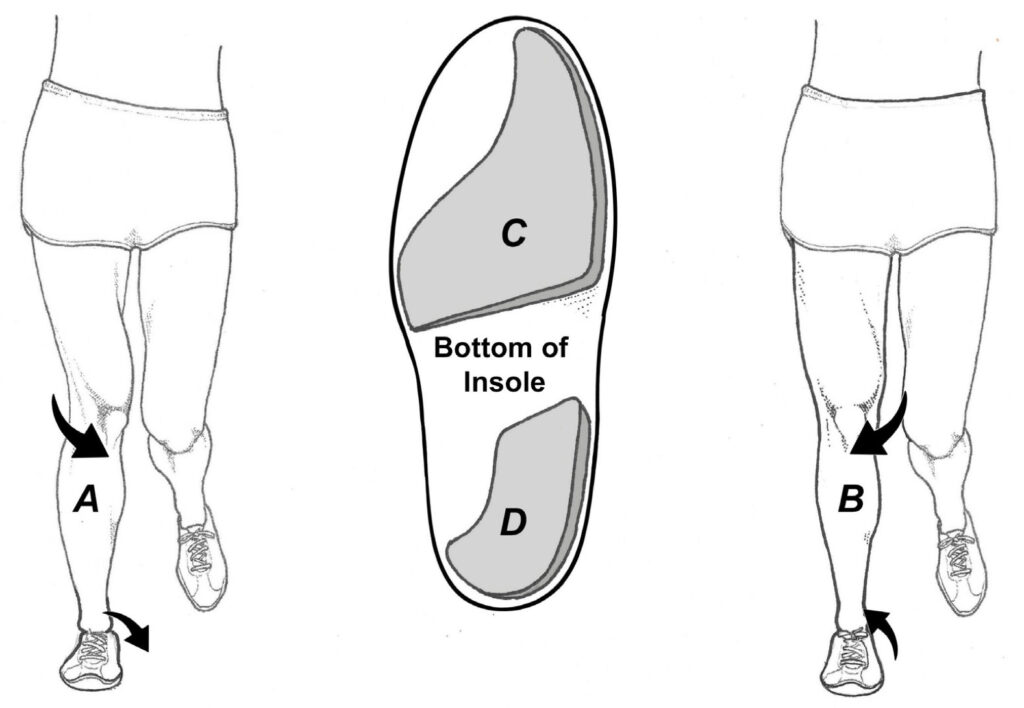
Fig. 3. By reducing the range of internal tibial rotation and decreasing the velocity of knee flexion, varus posts can reduce valgus collapse of the knee and ankle (A and B). The 2-piece Peel and Stick Varus Posts (C and D) allow you to post the forefoot and/or the rearfoot. A video reviewing exactly how to position the posts is available at www.humanlocomotion.com.
These findings are extremely important because excessive knee valgus on landing is strongly correlated with the development of a wide range of injuries, including anterior cruciate ligament tears. One of the more interesting aspects of this article is that the authors prescribed full length varus posts regardless of the patient’s foot architecture: both high and low arched individuals were treated with the same varus posts and had the same outcomes. The universal positive effect of varus posts is important because it takes the guesswork out of deciding which patients with valgus collapse might benefit the most from varus posts.
Interestingly, in an extensive 2018 literature review evaluating the ability of different components of an orthotic to alter lower limb movement patterns, researchers from the University of Montréal concluded that flat orthotics possessing arch support alone provided no control of lower extremity motion, while insoles possessing medial posting in either the rearfoot and/or forefoot significantly reduced foot pronation (15). The authors state that “us- ing medial posting is the most effective foot orthotic feature to reduce the peak rearfoot eversion and to control excessive foot pronation.” The findings of the 2018 literature review were corroborated in a 2019 study in which researchers evaluated 3-dimensional motion as subjects wore either a flat insole with an arch support, or the same insole possessing a 7° varus wedge (16). Results of this study conclusively prove that compared to insoles with arch support alone, wedged insoles more effectively reduce foot and ankle pronation, decrease internal rotation of the knee and hip, reduce hip adduction, and significantly lessen stress on the muscles responsible for decelerating pronation (16). The one caveat for using varus posts is that just as valgus posts can offload the medial knee, varus posts can increase pressure in the medial knee by causing the tibia to adduct in the frontal plane (16). As a result, varus posts should be used cautiously in individuals with medial knee osteoarthritis.
Taken together, the latest research shows that varus and valgus posts can play an important role in altering mechanics and/or preventing injuries. This is especially true for managing valgus collapse of the knee, lessening patellofemoral pressure, and/or improving alignment of the foot and leg. Unlike custom and over-the-counter orthotics, these posts do not physically support the arch, and will not cause disuse atrophy of the intrinsic muscles of the foot. Peel and Stick Posts are inexpensive, easy to apply, and should be a part of every practitioner’s clinical toolbox.
References:
- Perez-Morcillo A, et al. Association between the foot posture index and running related injuries: a case-control study. Clinical Biomech. 2019; 217-221.
- Mundemann A, Nigg B, Humble N, Stefanyshyn D. Orthotic comfort is related to kinematics, kinetics, and EMG in recreational runners, Med Sci Sports Exerc. 2003;35:1710–1719.
- McClinton S, Collazo C, Vincent E, et al. Impaired foot plantarflexor muscle performance in individuals with plantar heel pain and association with foot orthosis use. J Orthop Sports Phys Ther. 2016; 46:681-689.
- Protopapas K, Perry S. The effect of a 12-week custom foot orthotic intervention on muscle size and muscle activity of the intrinsic foot muscle of young adults during gait termination. Clinical Biomech. 2020; 78.
- T Sasaki, Yasudo K. Clinical Evaluation of the Treatment of Osteoarthritic Knees Using a Newly Designed Wedged Insole. Clin Orthop Related Res. 1987; 221:181-187.
- Butler RJ, Marchesi S, Royer T, Davis IS. The effect of a subject-specific amount of lateral wedge on knee mechanics in patients with medial knee osteoarthritis. J Orthop Res. 2007; 25:1121-1127.
- Hinman RS, Payne C, Metcalf BR, et al. Lateral wedges in knee osteoarthritis: what are their immediate clinical and biomechanical effects and can these predict a three-month clinical outcome?Arthritis Rheum (Arthritis Care Res). 2008; 59:408-415.
- Kuroyanagi Y, Nagura T, Matsumoto H, et al. The lateral wedged insole with subtalar strapping significantly reduces dynamic knee load in the medial compartment-gait analysis on patients with medial knee osteoarthritis. Osteoarthritis Cartilage. 2007; 15:932-936.
- Baker K, Goggins J, Xie H, et al. A randomized crossover trial of a wedged insole for treatment of knee osteoarthritis. Arthritis Rheum. 2007; 56:1198-1203.
- Toda Y, Segal N, Kato A, et al. Correlation between body composition and efficacy of lateral wedged insoles for medial compartment osteoarthritis of the knee. J Rheumatol. 2002; 29:541-545.
- Fisher DS, Dyrby CO, Mundermann A, et al. In healthy subjects without knee osteoarthritis, the peak knee adduction moment influences the acute effect of shoe interventions designed to reduce medialcompartment knee load. J Orthop Res. 2007; 25:540-546.
- Kogler G, Veer F, Solomonidis S, Paul J. The influence of medial and lateral placement of orthotic wedges unloading of the plantar aponeurosis. J Bone Joint Surg Am. 1999;81:1403-1413.
- Stackhouse CL, Davis IM, Hamill J. Orthotic intervention in forefoot and rearfoot strike running patterns. Clin Biomech (Bristol, Avon). 2004;19:64-70.
- Joseph M, Tiberio D, Baird J, et al. Knee valgus during drop jumps in national collegiate athletic Association Division I female athletes: the effect of a medial post. Am J Sports Med. 2008; 2:285-289.
- Desmyttere G, Hajizadeh M, Bleau J, et al. Effect of foot orthoses design on lower limb joint kinematics and kinetics during walking and flexible pes planovalgus: A systematic review and meta-analyses. Clinical Biomech. 2018; 59:117- 129.
- Braga U, Mendonca L, Mascarenhaus R, et al. Effects of medially wedged insoles on the biomechanics of the lower limbs of runners with excessive foot pronation and foot varus alignment. Gait and Posture 2019; 74:242-249.
- Hinman R, Bennell K. Advances in insoles and shoes for knee arthritis. Curr Opin Rheumatol 2009; 21:164 – 170.
- Chang A, Hayes K, et al. Hip abduction moments and protection against medial tibiofemoral osteoarthritis progression. Arth Rheum. 2005;52:3515-3519.