
Weakness of the intrinsic toe flexors, specifically the flexor digitorum brevis muscle (FDB), is a common and underappreciated cause of a wide range of injuries. In 2015, Sullivan et al. (1) examined 202 people with chronic heel pain and compared them to 70 asymptomatic people and determined that weakness of the toe flexors was a common finding in the heel pain group. This is consistent with research showing that heel spurs do not form at the origin of the plantar fascia as popularly believed, they form at the attachment point of FDB (2). Researchers suggest that in an attempt to offload the neighboring plantar fascia, FDB fires with more force and the resultant tensile strain leads to the development of a traction bone spur on the calcaneus. Over time, the bone spur gradually becomes a weight bearing point capable of creating its own set of symptoms.
Because FDB supports the arch and allows for the transfer of force from the rearfoot to the forefoot during pushoff, maintaining strength in this muscle is important not just for injury prevention, but also for improved athletic performance. In 2017, Paquette et al. (3) proved that arch weakness strongly correlated with impaired running performance as we age. More recently, Yuasa et al. (4) had college athletes perform agility tasks and determined that the quickest athletes had the strongest toes. Because soccer players change direction 700 times in a single game (5), even a slight improvement in toe strength could result in substantial improvements in agility and speed.
While toe strength can be measured with dynamometers and/or the paper grip test, the easiest way to evaluate strength in the FDB is by instructing a standing patient to push their toes into the floor with as much force as possible. When FDB is weak, their second through fifth toes remain stationary while the distal phalanx plantarflexes (Fig. 1B). Conversely, when FDB is strong, the intermediate phalanx plantarflexes, creating a visible crease between the intermediate and distal phalanx, which I refer to as a “positive wink sign” (Fig. 1A). A negative or absent wink sign typically indicates weakness not just of the FDB, but of all the intrinsic muscles of the arch.
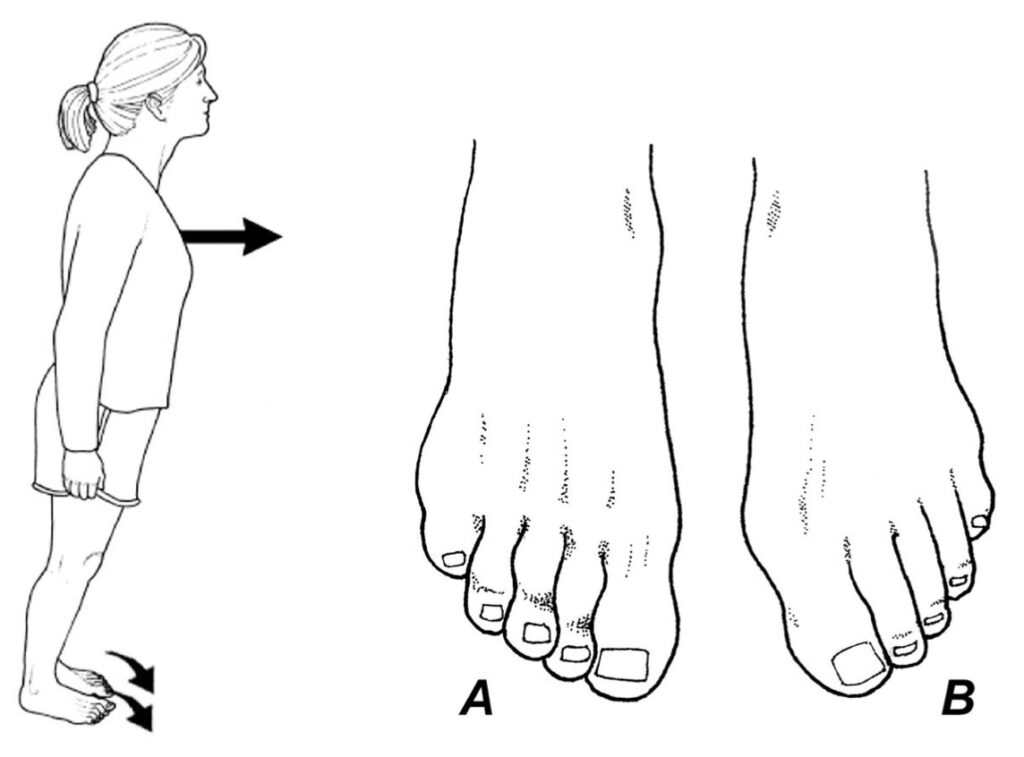
A positive wink sign is present when you see a clear crease form at the distal interphalangeal joint (A). In this illustration, the left FDB is weak and there is no visible crease present on the dorsal aspect of the distal interphalangeal joint (B).
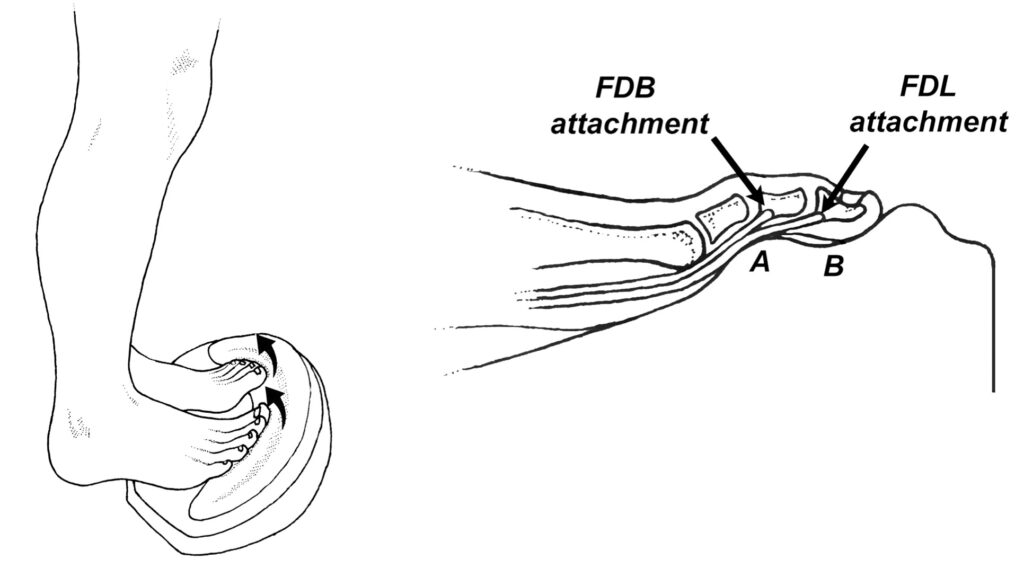
The reason the wink sign occurs is because of the interesting relationship between FDB and longus. Just prior to attaching to the intermediate phalanx, the tendon of FDB splits, attaching to the plantar medial and lateral sides of the intermediate phalanx (Fig 2A). The flexor digitorum longus tendon runs deep to FDB tendons and attaches to the distal phalanx by running directly through the bifurcated FDB tendons (Fig. 2B). When someone with a weak FDB attempts to plantarflex their toes, flexor digitorum longus takes over, driving the tips of the toes into the ground. This action results in reduced contact between the ground and the toes, limiting the ability to generate force (Fig. 2C). When FDB is strong, the intermediate phalanx plantarflexes, allowing the toes to make greater ground contact (Fig. 2D), which in turn allows for greater force output and possibly even enhances proprioception. The increased digital ground contact present when FDB is activated may explain why a strong FDB is so important with athletic performance: during terminal pushoff while running or jumping, force is centered beneath the toes, not the metatarsal heads, explaining why the best athletes have the strongest toes. In support of this theory, researchers have shown the world’s fastest sprinters have significantly longer toes than their sub-elite competitors, which increases the lever afforded the long and short digital flexors, resulting in increased force production beneath the toes and significantly faster running times (6,7).
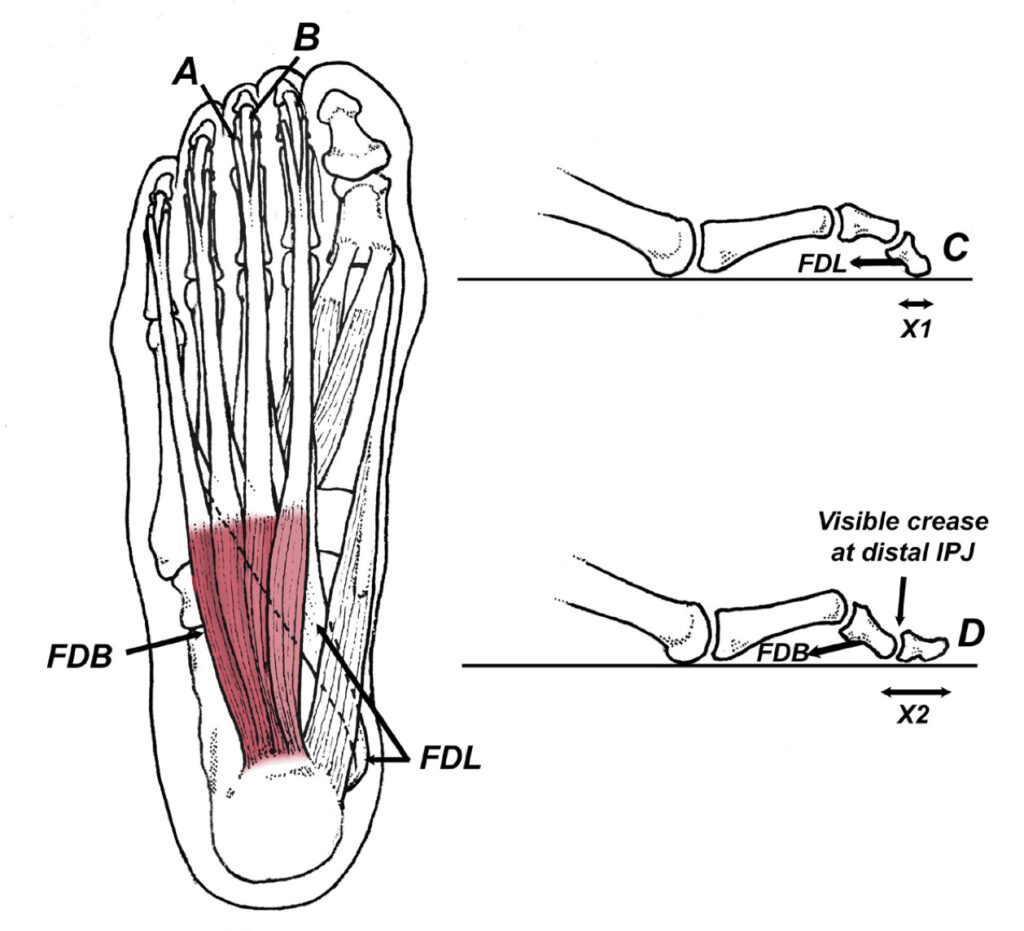
The flexor digitorum longus muscle (FDL) travels deep to the FDB, and its tendon inserts into the basis of the distal phalanges (B). When someone with weakness of the FDB attempts to push their second through fifth toes into the ground, FDL takes over and the distal interphalangeal joint plantarflexes (C). In contrast, individuals with strong FDBs create a visible crease along the dorsal aspect of the interphalangeal joint as FDB plantarflexes the proximal interphalangeal joint (D). A strong FDB pulls the distal toe directly against the ground, increasing ground contact and the ability to generate force (compare X1 to X2).
If you do not have access to a toe strength dynamometer, the wink sign is a useful clinical tool for identifying weakness of the intrinsic muscles of the arch, specifically FDB. When a positive wink sign is absent, all of the arch muscles should be aggressively strengthened with a ToePro exercise platform. This platform has an elevated support built beneath the insertions of flexor digitorum longus and brevis, which forces you to recruit these muscles while they are in a stretched position (Fig. 3). As demonstrated by Goldmann et al. (8), exercising your toes while they are actively lengthened produces 4-times the strength gains associated with conventional exercises, such as elastic band exercises and marble pickups. Just 6 weeks of performing isometric toe exercises with the toes stretched resulted in significant increases in horizontal jump distance (8). This compares to six months of training with elastic bands and marble pickups, which resulted in no appreciable increase in the ability to bear weight beneath the toes (9). Apparently, because strength gains are angle specific, in order to be effective, the toe muscles must be exercised in the upward positions they are in while walking, running, and jumping.
References:
- Sullivan J, et al. Musculoskeletal and activity-related factors associated with plantar heel pain. Foot & Ankle Int. 2015; 36:37–45.
- Abreu M, Chung C, Mendes L, et al. Plantar calcaneal enthesophytes: new observations regarding sites of origin based on radiographic, MR imaging, anatomic, and paleopathologic analysis. Skeletal Radiol. 2003;32:13-21.
- Paquette M, DeVita P, Williams D. Biomechanical implications of training volume and intensity in aging runners. Med Sci Sports Exerc. 2017: October 9.
- Yuasa Y, Kurihara T, Isake T. Relationship between the toe muscular strength and the ability to change direction in athletes. J Human Kinetics. 2018; 64:47– 55.
- Bloomfield J, Polman R, O’ Donoghue P. Physical demands of different positions in FA Premier League soccer. J Sport Sci Med, 2007; 6: 63–70.
- Lee S, Piazza S. Built for speed: musculoskeletal structure and sprinting ability. J Exper Biol. 2009;212:3700-3707.
- Tanaka T, Suga T, Otsuka M, et al. Relationship between the length of the forefoot bones and performance in male sprinters. Scand J Med Sci Sports. 2017;1–8.
- Goldmann J, Sanno M, Willwacher S, et al. The potential of toe flexor muscles to enhance performance. Journal of Sports Sciences. 2013;31:424-433.
- Spink, M.J., et al. Effectiveness of a multifaceted podiatry intervention to prevent falls in community dwelling older people with disabling foot pain: randomized controlled trial. BMJ.2011;342:d3411.
- Mickle, K, et al., ISB Clinical Biomechanics Award 2009: Toe weakness and deformity increase the risk of falls in older people. Clinical Biomechanics. 2009;24:787-791.