
Summary
- Interdigital neuromas are common, poorly studied, and notoriously difficult to treat.
- By offloading the third and fourth metatarsal heads throughout propulsion, the new Peel and Stick interdigital neuroma balance allows you to effectively treat interdigital neuromas, usually without the need for surgery and/or expensive orthotics.
Also known as Morton’s neuroma, interdigital neuromas result from entrapment of one or more of the interdigital nerves, which are branches of the medial and lateral plantar nerves (Fig. 1). This painful forefoot condition affects women four times more often than men, particularly women in their 50s and 60s. The most common early symptoms include tingling between the toes and a feeling of fullness between the involved metatarsal heads. Affected individuals frequently complain that their socks are “bunched” in the forefoot and that the discomfort is reduced when the shoes are removed. Over time, a thick neuroma may form that increases the likelihood of chronicity because the thickened nerve is more readily pinched.
Clinically, it is often possible to identify a neuroma by squeezing the forefoot at the metatarsal heads and feeling for the presence of a Mulder’s click: a clunk-like sound that can be palpated, which occurs when a swollen bursa is displaced into the neuroma (Fig. 2). Mulder’s click is extremely important when diagnosing interdigital neuritis, as it has a 94 to 98% sensitivity (1). Other important clinical signs include the fact that interdigital neuromas do not produce pain on the metatarsal heads themselves, and are frequently associated with a slight increase in the interdigital space (Fig. 3). Physical examination is the key to diagnosing Morton’s neuroma, as ultrasound and MRI are notoriously unreliable (2,3).
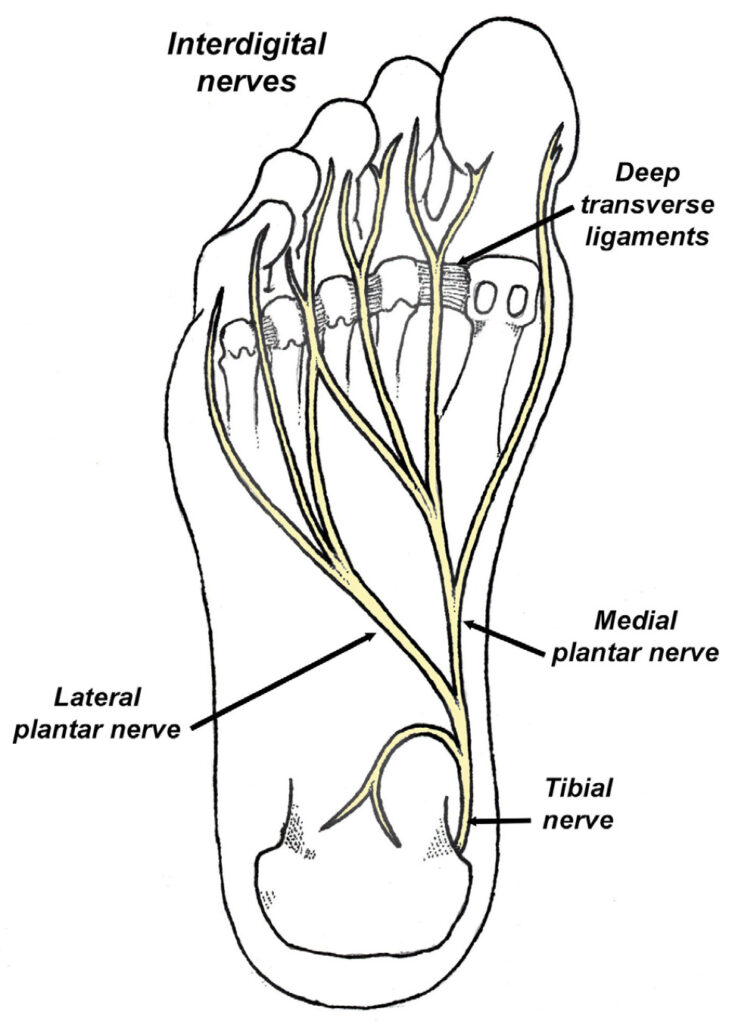

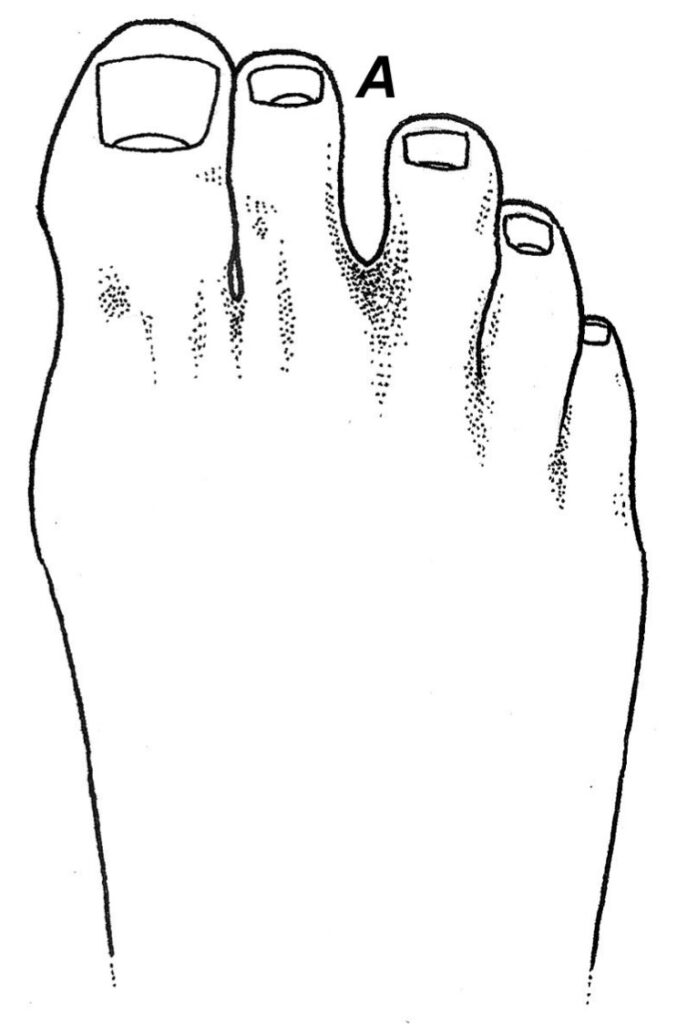
Fig. 3. The toes are often separated at the interspace affected by an interdigital neuroma (A).
While this condition may occur at any of the interdigital nerves, the nerves located in the second and third interspace produce pain in 32% and 66% of patients respectively. Interdigital nerve injuries do not occur between the first and second metatarsal heads and occur in only 2% of cases between the fourth and fifth metatarsal (4). Although it was originally suggested that the nerve between the third and fourth metatarsal heads were more often involved because it receives fibers from both the medial and lateral plantar nerves (which was believed to make it thicker), this theory has been disproved since all of the interdigital nerves are approximately the same diameter (5).
Until recently, the most popular theory regarding the origin of interdigital neuritis was that dorsiflexion of the toes during propulsion tractioned the interdigital nerves against the deep transverse ligament, damaging the interdigital nerve fibers. Based on this theory, metatarsal pads were prescribed to lift the metatarsal heads off the transverse ligament, and/or surgery was performed to section the transverse ligament. Unfortunately, these interventions were rarely successful because it was not the transverse ligament that was damaging the interdigital nerves.
To identify the exact etiology of interdigital neuromas, Kim et al. (5), performed meticulous dissections on 17 fresh frozen cadavers to evaluate the relationship between interdigital neuromas and the surrounding soft tissues. Upon dissection, the authors concluded that the nerve is not compressed beneath the deep transverse ligament, rather, the interdigital nerve is compressed beneath the distal aspect of the involved metatarsal head and its proximal phalanx (Fig. 4). Kim’s research explains why metatarsal pads and bar posts have been so ineffective in managing Interdigital neuromas: they do not support the proper location. To be effective, the distal aspects of the third and fourth metatarsal heads must be offloaded during terminal propulsion.
To specifically offload irritated neuromas, the Peel and Stick Interdigital Balance was developed to simultaneously support the first, second, and fifth metatarsal heads, and most importantly, the entire hallux and second toe (Fig. 5). Supporting the entire medial forefoot is the key to success with the Peel and Stick Balance, because it allows for a constant offloading of the third and fourth metatarsal heads throughout pushoff. This balance is thick and durable, as it contains one layer of urethane rubber with a self-stick back, one layer of EVA foam for pressure distribution, and a protective synthetic suede cover that resists wear and tear.
To apply the interdigital balance, mark the location of a patient’s second and fifth metatarsal heads on the bottom of their insoles. Remove the self-stick back and place the balance on the bottom of the insole so the fifth metatarsal head is supported by the lateral side of the balance, and the second metatarsal head and corresponding toe is supported on the medial side. The third and fourth metatarsal heads should not be supported by the balance, but the balance is very close to the proximal aspects of these metatarsal heads. Trim any overhanging edges with scissors and place it in the patient’s shoe. It’s that easy.
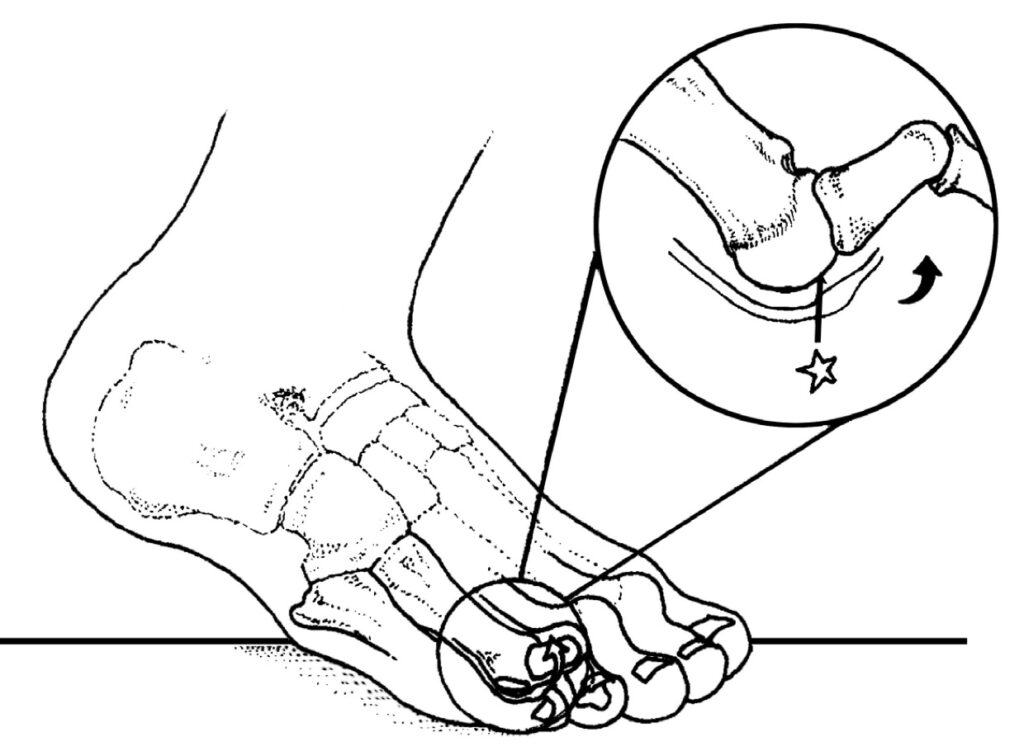
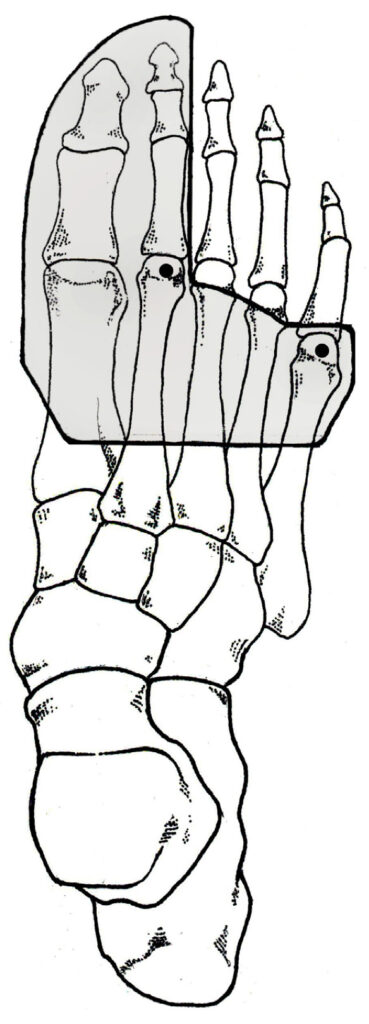
Fig. 5. The Peel and Stick Interdigital Balance supports the first and second toes, along with the first, second, and fifth metatarsal heads (dots). The balance extends just short of the third and fourth metatarsal heads. By sup- porting the medial forefoot, the interdigital nerve is offloaded during propulsion, when the nerve is at greatest risk of being compressed.
If needed, additional conservative interventions should be considered, such as mobilizing restricted joints of the foot/ankle, nerve glide techniques, and/or restoration of ankle dorsiflexion by stretching gastrocnemius (6). Because more than one in five surgical cases for interdigital neuromas fail, and as many as 40% of revision surgeries for interdigital neuromas fail (1), comprehensive conservative care is the best option, and should be initiated as soon as symptoms begin as the longer the nerve is compressed, the worse the prognosis.
References:
- Caprio F, Meringolo R, Eddine S, et al. Morton’s interdigital neuroma of the foot: A literature review. Foot Ankle Surg. 2018; 24:92-98.
- Symeonidis P, Iselin L, Simmons N, et al. Prevalence of interdigital nerve enlargements in an asymptomatic population. Foot Ankle Int. 2012;33:543–7.
- Torres-Claramunt R, Ginés A, Pidemunt G, et al. MRI and ultrasonography in Morton’s neuroma: diagnostic accuracy and correlation. Indian J Orthop. 2012;46:321–5.
- Kasparek M, Schneider W. Surgical treatment of Morton’s neuroma: clinical results after open excision. Int Orthop. 2013;37:1857–61.
- Kim J, Choi J, Park J, et al. An anatomical study of Morton’s interdigital neuroma: the relationship between the occur- ring site and the transverse metatarsal ligament (DTML). Foot Ankle Int. 2007;28:1007-1010.
- Michaud T. Human Locomotion: The Conservative Management of Gait-related Disorders. Newton Biomechanics, Newton, Massachusetts;2012.