
Each year, nearly 2 million Americans seek medical attention for a painful heel. In the US alone, the annual economic cost for managing this common condition is in excess of $300 million (1). While the majority of patients with painful heels respond favorably within 3 months, nearly 10% of patients with painful heels become chronic, experiencing pain and limited function for more than 2 years after the initial diagnosis.
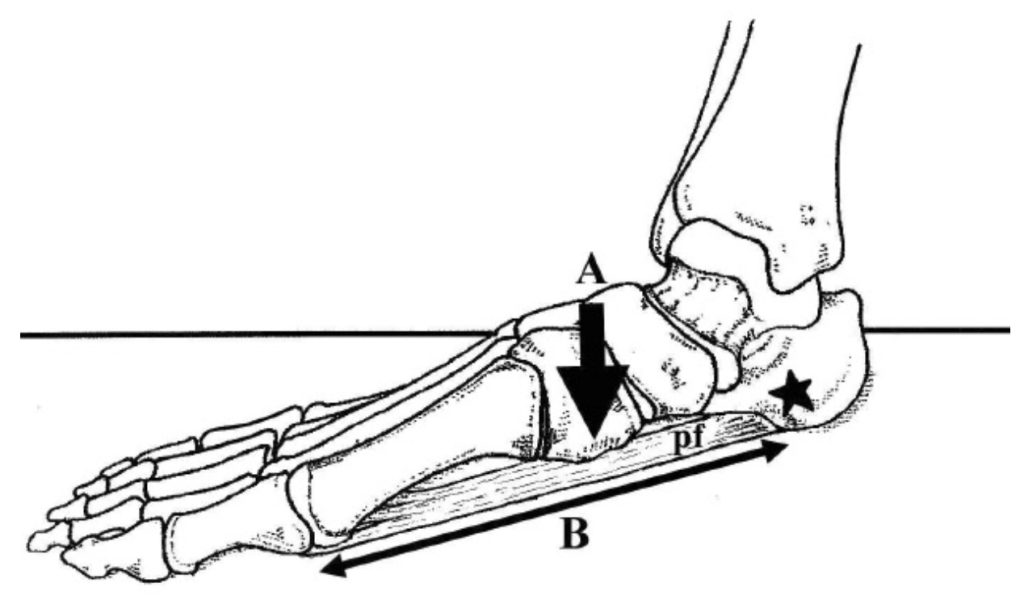
Until recently, it was believed the most common cause of heel pain was an over-pronated foot. The logical assumption was lowering of the arch increased tensile strain on the plantar fascia causing chronic pain at the attachment of the plantar fascial to the calcaneus (Fig. 1). Because excessive lowering of the arch is so often managed with arch supports, orthotic intervention eventually became one of the most popular methods of managing chronic heel pain.
While orthotic intervention is effective for reducing pain in a wide range of conditions (2), recent research shows that orthotics are not that effective for managing heel pain. In a comprehensive 2018 meta-analysis by Whittaker et al. (3), both over-the-counter and custom orthotics produced insignificant reductions in plantar heel pain when compared to sham orthotics. The reason for the surprising outcome is that excessive lowering of the arch and the development of heel pain are not that strongly correlated (4-6).
To determine which biomechanical and activity-related factors might be associated with heel pain, Sullivan et al. (4) took 202 people with plantar heel pain and compared them to 70 asymptomatic control participants. The authors evaluated a wide range of causes for heel pain, including body mass index, foot and ankle muscle strength, calf endurance, ankle and first metatarsophalangeal joint dorsiflexion, foot alignment, occupational standing time, exercise level, and generalized hypermobility. As with other studies, Sullivan et al. (4) found that a more pronated foot was in no way correlated with the development of plantar heel pain. Additionally, chronic heel pain was not associated with tibialis posterior weakness, rearfoot eversion range of motion, dorsiflexion of the first metatarsophalangeal joint, generalized hypermobility, occupational standing time or even exercise level. The only factors that correlated with the development of heel pain were limited ankle dorsiflexion (measured both with knee straight and bent), weakness of the toe flexors, and weakness of the peroneal musculature. The authors of the study emphasize that because these 3 factors are modifiable, they should be targeted in the management of plantar heel pain.
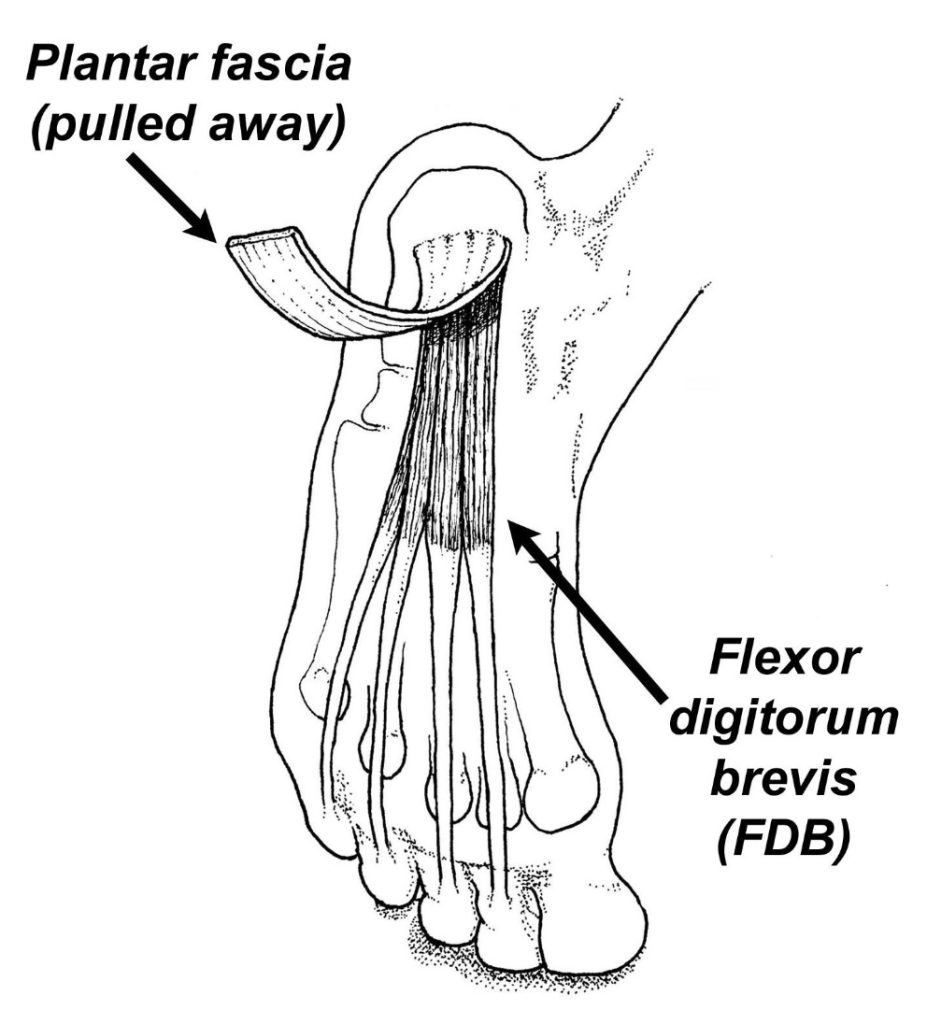
The observation by Sullivan et al. (4) that limited ankle dorsiflexion correlated with the development of heel pain was not surprising. Numerous studies have demonstrated that calf tightness correlates with the development of heel pain and that stretching is an effective form of managing chronic heel pain (7,8). It was also not surprising that heel pain patients also had weakness of their toe flexors. Wearing et al. (5) identified toe weakness as a possible cause/effect of chronic heel pain almost 15 years ago. Because flexor digitorum brevis can unload the plantar fascia during propulsion (Fig. 2), strengthening the toe muscles should be an integral part in the management of heel pain.
The big surprise of the study was that peroneal strength so strongly correlated with heel pain. In fact, heel pain patients had eversion strength differences more than twice the effect size of any other strength deficit. Until this paper came out in 2015, no other paper had ever evaluated peroneal strength in heel pain patients. It is likely that peroneus longus plays the key role of plantarflexing the first metatarsal (Fig. 3), thereby unloading the medial band of the plantar fascia. The reduced strain placed on the plantar fascia associated with a strong peroneus longus contraction may limit the tensile strain transferred into the calcaneus.
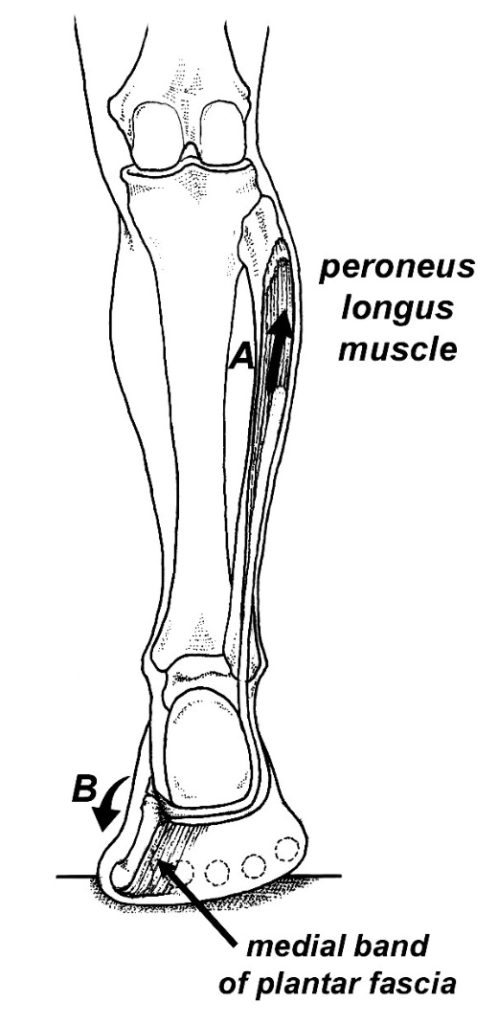
Fig. 3. Concentric contraction of the peroneus longus muscle (A) plantarflexes the first metatarsal during propulsion (B), thereby reducing strain on the medial band of the plantar fascia.
Since toe flexor and peroneal weakness are so strongly correlated with the development of heel pain, it is important to identify which exercises most effectively strengthen these 2 key muscle groups. Unfortunately, popular exercises such as the short foot exercise, marble pickups, and various elastic band exercises have been proven to produce negligible increases in toe flexor strength (9,10). In contrast, Goldmann et al. (11) recently demonstrated that exercising the toe muscles while they are in a stretched position produces dramatic increases in toe flexor strength. These authors had 15 subjects perform 4 sets of 5 isometric contractions (3-second contractions performed at 90% full effort with the toes dorsiflexed 25 degrees), 4 times per week for 7 weeks. At the end of the study, the subjects had toe flexor strength increases of nearly 40%, along with appreciable improvements in their horizontal jump distance. The authors theorized that maintaining the toe muscles in a stretched position during the isometric contractions created an “optimal overlap of the contractile elements” thereby allowing for enhanced muscle hypertrophy. Prior research has also shown that exercising muscles in their lengthened positions produces significantly greater strength gains than exercising the same muscles while they are in their midline or shortened positions (12).
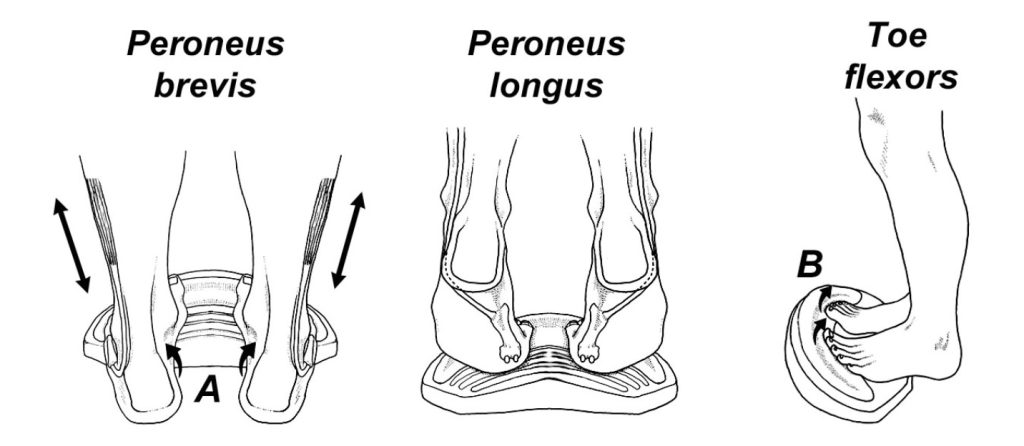
The easiest way to strengthen both the toe flexors and peroneals in their lengthened positions is with the ToePro exercise platform. This platform has a built-in elevation beneath the toes to duplicate the dorsiflexion angles used in the study by Goldmann et al. (9). The device also has a negative lateral slant that places the peroneal muscles in their lengthened positions (Fig. 4). Performing 4 sets
of 25 repetitions 3 times per week very effectively strengthens the peroneal and toe muscles. Each exercise session should be completed by performing a 60-second stretch where you rest your heels off the back of the ToePro device. By stretching and strengthening the muscles proven to be correlated with chronic heel pain, the ToePro exercise device allows you to target muscles most likely to be causing your chronic heel pain. Each exercise session takes about 5 minutes to complete and 300% strength gains in the first 12 weeks are common. Those are impressive strength gains that are difficult to achieve with conventional foot and ankle exercises.
References:
- Tong KB, Furia J. Economic burden of plantar fasciitis treatment in the United States. Am J Orthop. 2010;39(5):227-231
- Malkin K, et al. A year of foot and ankle orthotic provision for adults: Prospective consultations data, with patient satisfaction survey. The Foot. 2008;18:75-83.
- Whittaker GA, Munteanu SE, Menz HB, et al. Foot orthoses for plantar heel pain: a systematic review and meta-analysis. Br J Sports Med 2018;52:322–8.
- Sullivan J, et al. Musculoskeletal and activity-related factors associated with plantar heel pain. Foot & Ankle International. 2015, Vol. 36(1) 37 –45.
- Wearing SC, Smeathers JE, Yates B, et al. Sagittal movement of the medial longitudinal arch is unchanged in plantar fasciitis. Med Sci Sports Exerc. 2004;36:1761-1767
- Allen RH, Gross MT. Toe flexors strength and passive extension range of motion of the first metatarsophalangeal joint in individuals with plantar fasciitis. J Orthop Sports Phys Ther. 2003;33:468-478.
- Riddle DL, Pulisic M, Pidcoe P, Johnson RE. Risk factors for plantar fasciitis: a matched case-control study.
J Bone Joint Surg Am. 2003;85A(5):872-877. - DiGiovanni B, Nawoczenski D, Lintal M, et al. Tissue specific plantar fascia-stretching exercise enhances
outcomes in patients with chronic heel pain. A prospective, randomized study. J Bone Joint Surg. 2003;85-
A:1270–1277. - Houck J, Seidl L, Montgomery A. Can foot exercises alter foot posture, strength, and walking foot pressure
patterns in people with severe flat foot? Foot & Ankle Orthopaedics. September 18, 2017. - Spink, M.J., et al. Effectiveness of a multifaceted podiatry intervention to prevent falls in community
dwelling older people with disabling foot pain: randomized controlled trial. BMJ, 2011; 342:d3411. - Goldmann J, Maximilian Sanno, Steffen Willwacher, et al. The potential of toe flexor muscles to enhance
performance, Journal of Sports Sciences. 2012;31:424-433. - Noorkoiv M, Kazunori K, Blazevich A. Neuromuscular adaptations associated with knee joint angle-specific
force change. Med Sci Sports Exerc. 2014;46:1525–1537.